The greatest irony in global health is that the poorest countries carry the largest disease burden. If we resize the countries of the globe in proportion to the subject of interest, we see that Sub-Saharan Africa is the worst hit region by HIV/AIDS. This is the most devastating epidemic of our time. We also see that this region has the least capability in terms of dealing with the disease. There are very few doctors and, quite frankly, these countries do not have the resources that are needed to cope with such epidemics.
De grootste ironie in de wereldwijde gezondheidszorg is dat de armste landen de grootste ziektelast te dragen hebben. Als we de grootte van de landen op de wereldkaart in verhouding tot dit onderwerp aanpassen zien we dat Afrika bezuiden de Sahara het zwaarst door HIV/AIDS getroffen is. Dit is de meest verwoestende epidemie van onze tijd. We zien ook dat deze regio de minste mogelijkheden heeft om de ziekte te behandelen. Er zijn zeer weinig artsen en deze landen hebben, eerlijk gezegd, niet de middelen om het hoofd te bieden aan zulke epidemieën.
So what the Western countries, developed countries, have generously done is they have proposed to provide free drugs to all people in Third World countries who actually can't afford these medications. And this has already saved millions of lives, and it has prevented entire economies from capsizing in Sub-Saharan Africa.
Westerse landen, ontwikkelde landen, hebben genereus gratis medicijnen verstrekt aan alle mensen in Derde Wereld landen die zich deze medicijnen niet kunnen veroorloven. En dit heeft reeds miljoenen levens gered en het heeft verhinderd dat hele economieën in sub-Sahara Afrika over de kop gingen.
But there is a fundamental problem that is killing the efforts in fighting this disease, because if you keep throwing drugs out at people who don't have diagnostic services, you end up creating a problem of drug resistance. This is already beginning to happen in Sub-Saharan Africa. The problem is that, what begins as a tragedy in the Third World could easily become a global problem. And the last thing we want to see is drug-resistant strains of HIV popping up all over the world, because it will make treatment more expensive and it could also restore the pre-ARV carnage of HIV/AIDS.
Maar er is een fundamenteel probleem dat de inspanningen in de strijd tegen deze ziekte teniet doet. Als je blijft doorgaan met geneesmiddelen uitdelen aan mensen, die niet over diagnostische diensten beschikken, dan creëer je uiteindelijk een probleem van resistentie tegen geneesmiddelen. Dit is al aan het gebeuren in Afrika bezuiden de Sahara. Het probleem is dat, wat als een tragedie in de Derde Wereld begint, gemakkelijk kan uitgroeien tot een wereldwijd probleem. En het laatste wat we willen zien is dat resistente HIV-stammen over de hele wereld gaan opduiken. Dat zal de behandeling duurder maken en opnieuw leiden tot een bloedbad van HIV/AIDS zoals in de tijd van voor de antiretrovirale middelen .
I experienced this firsthand as a high school student in Uganda. This was in the 90s during the peak of the HIV epidemic, before there were any ARVs in Sub-Saharan Africa. And during that time, I actually lost more relatives, as well as the teachers who taught me, to HIV/AIDS. So this became one of the driving passions of my life, to help find real solutions that could address these kinds of problems.
Ik heb dit als middelbareschoolstudent in Uganda zelf meegemaakt. Dat was in de jaren '90 tijdens de piek van de HIV-epidemie, voordat er enig antiretroviraal middel in sub-Sahara Afrika te vinden was. Ik heb toen meerdere familieleden en leraren verloren aan HIV/AIDS. Het werd een van de drijvende passies in mijn leven om echte oplossingen te vinden voor dit soort problemen.
We all know about the miracle of miniaturization. Back in the day, computers used to fill this entire room, and people actually used to work inside the computers. But what electronic miniaturization has done is that it has allowed people to shrink technology into a cell phone. And I'm sure everyone here enjoys cell phones that can actually be used in the remote areas of the world, in the Third World countries. The good news is that the same technology that allowed miniaturization of electronics is now allowing us to miniaturize biological laboratories.
We zijn allemaal op de hoogte van de wonderen van de miniaturisatie. Vroeger vulden computers hele kamers en werkten mensen daadwerkelijk binnen in de computers. Elektronische miniaturisering liet ons toe die technologie te verkleinen tot de grootte van een mobiele telefoon. Iedereen hier geniet van de toepassing van mobiele telefoons. Maar die zijn ook bruikbaar in de meest afgelegen gebieden van de wereld, in de Derde Wereld landen. Het goede nieuws is dat dezelfde technologie die miniaturisering van elektronica met zich meebracht, ons nu ook de mogelijkheid geeft biologische laboratoria te miniaturiseren.
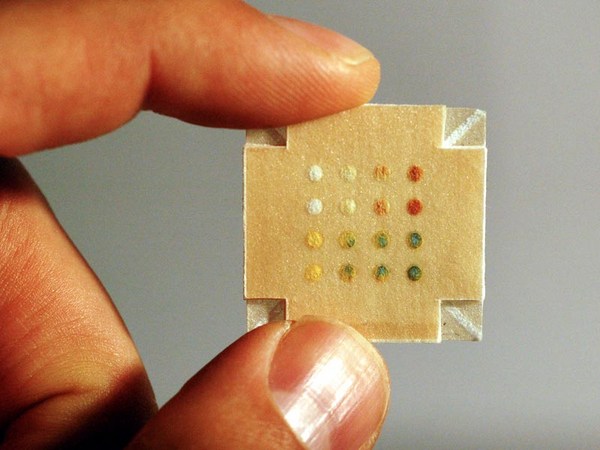
So, right now, we can actually miniaturize biological and chemistry laboratories onto microfluidic chips. I was very lucky to come to the US right after high school, and was able to work on this technology and develop some devices. This is a microfluidic chip that I developed. A close look at how the technology works: These are channels that are about the size of a human hair -- so you have integrated valves, pumps, mixers and injectors -- so you can fit entire diagnostic experiments onto a microfluidic system.
We kunnen nu biologische en chemische laboratoria miniaturiseren op microfluïdische chips. Ik had het geluk om direct na de middelbare school naar de VS te kunnen komen. Daardoor kon ik aan deze technologie werken en aan de ontwikkeling van enkele apparaten. Dit is een microfluïdische chip die ik heb ontwikkeld. Een korte blik op hoe de technologie werkt: dit zijn kanalen ongeveer ter grootte van een menselijk haar. Je ziet geïntegreerde kleppen, pompen, mixers en injectoren. Je kunt hele diagnostische experimenten op een microfluïdisch systeem realiseren.
So what I plan to do with this technology is to actually take the current state of the technology and build an HIV kit in a microfluidic system. So, with one microfluidic chip, which is the size of an iPhone, you can actually diagnose 100 patients at the same time. For each patient, we will be able to do up to 100 different viral loads per patient. And this is only done in four hours, 50 times faster than the current state of the art, at a cost that will be five to 500 times cheaper than the current options. So this will allow us to create personalized medicines in the Third World at a cost that is actually achievable and make the world a safer place.
Ik heb het plan opgevat om met deze technologie in haar huidige stand van ontwikkeling een HIV-kit te bouwen in een microfluïdisch systeem. Met één microfluïdische chip, ter grootte van een iPhone, kan je nu 100 patiënten tegelijkertijd diagnosticeren. Voor iedere patiënt zullen we in staat zijn om tot 100 verschillende virale belastingen te onderzoeken. En dat in vier uur tijd. 50 keer sneller dan met de huidige stand van de techniek. Tegen een kostprijs die 5 tot 500 keer goedkoper dan de huidige zal zijn. Dit zal ons toelaten om in de Derde Wereld gepersonaliseerde medicijnen te creëren tegen een haalbare kostprijs. En zo van de wereld een veiliger plaats maken.
I invite your interest as well as your involvement in driving this vision to a point of practical reality.
Ik hoop op jullie interesse en betrokkenheid om deze droom praktische werkelijkheid te laten worden.
Thank you very much.
Dank u zeer.
(Applause)
(Applaus)