The greatest irony in global health is that the poorest countries carry the largest disease burden. If we resize the countries of the globe in proportion to the subject of interest, we see that Sub-Saharan Africa is the worst hit region by HIV/AIDS. This is the most devastating epidemic of our time. We also see that this region has the least capability in terms of dealing with the disease. There are very few doctors and, quite frankly, these countries do not have the resources that are needed to cope with such epidemics.
Globalinės sveikatos didžiausia ironija yra ta, jog vargingiausios šalys neša didžiausią ligų naštą. Jei mes permatuotume Žemės rutulio šalių dydį remdamiesi domėjimosi subjektu, pamatytume, kad Afrikoje į pietus nuo Sacharos yra daugiausia ŽIV/AIDS susirgimo atvejų. Tai yra mūsų laiko labiausiai triuškinanti epidemija. Taip pat pamatytume, jos šis regionas yra mažiausiai pajėgus susidoroti su šiomis ligomis. Ten yra labai nedaug daktarų ir, atvirai kalbant, šios šalys neturi pakankamai išteklių, kurių reikia norint susidoroti su tokiomis epidemijomis.
So what the Western countries, developed countries, have generously done is they have proposed to provide free drugs to all people in Third World countries who actually can't afford these medications. And this has already saved millions of lives, and it has prevented entire economies from capsizing in Sub-Saharan Africa.
Taigi ką Vakarų šalys, išsivysčiusios šalys, kilniaširdiškai padarė yra tai, kad jos pasiūlė tiekti nemokamus vaistus visiems trečio pasaulio šalių žmonėms, kurie iš tikrųjų neišgali jų įsigyti. Ir tai iš tikrųjų jau išgelbėjo milijonus gyvybių ir apsaugojo ištisas Afrikos į pietus nuo Sacharos ekonomijas nuo apvirtimo.
But there is a fundamental problem that is killing the efforts in fighting this disease, because if you keep throwing drugs out at people who don't have diagnostic services, you end up creating a problem of drug resistance. This is already beginning to happen in Sub-Saharan Africa. The problem is that, what begins as a tragedy in the Third World could easily become a global problem. And the last thing we want to see is drug-resistant strains of HIV popping up all over the world, because it will make treatment more expensive and it could also restore the pre-ARV carnage of HIV/AIDS.
Tačiau yra esminė problema, kuri žudo visas kovos su šiomis ligomis pastangas. Nes, jei tu vis mėtysi į žmones vaistus, kurie neturi prieigos prie diagnostinių paslaugų, pabaigoje tu tik sukursi atsparumo vaistams problemą. Tai jau prasideda Afrikoje į pietus nuo Sacharos. Problema yra ta, kad kas prasideda trečiajame pasaulyje kaip tragedija labai lengvai gali tapti globaline problema. Ir paskutinis dalykas, kurį norime matyti, tai atsparios vaistams ŽIV atmainos, netikėtai atsirandančios visame pasaulyje, nes tai padarytų gydymą dar brangesnį ir taip pat galėtų sugrąžinti pre-ARV ŽIV/AIDS skerdynes.
I experienced this firsthand as a high school student in Uganda. This was in the 90s during the peak of the HIV epidemic, before there were any ARVs in Sub-Saharan Africa. And during that time, I actually lost more relatives, as well as the teachers who taught me, to HIV/AIDS. So this became one of the driving passions of my life, to help find real solutions that could address these kinds of problems.
Pirmąkart su tuo susidūriau besimokydamas gimnazijoje Ugandoje. Tai buvo devintame dešimtmetyje per pačią ŽIV epidemijos kulminaciją, dar prieš atsirandant ARV Afrikoje į pietus nuo Sacharos. Tuo metu, aš praradau daugiau giminių, taip pat kaip ir mokytojai, kurie mane mokė, dėl ŽIV/AIDS. Taigi tai tapo viena mano gyvenimo aistrų, padėti rasti sprendimus būtent tokioms problemoms spręsti.
We all know about the miracle of miniaturization. Back in the day, computers used to fill this entire room, and people actually used to work inside the computers. But what electronic miniaturization has done is that it has allowed people to shrink technology into a cell phone. And I'm sure everyone here enjoys cell phones that can actually be used in the remote areas of the world, in the Third World countries. The good news is that the same technology that allowed miniaturization of electronics is now allowing us to miniaturize biological laboratories.
Visi žinome miniatiūrizacijos stebuklą. Seniau kompiuteris užimdavo atskirą kambarį, o žmonės iš tiesų dirbdavo kompiuterio viduje. Bet elektroninė miniatiūrizacija leido žmonėms sumažinti technologijas iki mobiliojo telefono. Ir aš esu isitikinęs, kad visi čia esantys džiaugiasi mobiliaisiais telefonais, kuriais išties galima naudotis tolimose pasaulio vietovėse, trečiojo pasaulio šalyse. Geros naujienos, kad tokia pati technologija, kuri leido miniatiūrizuoti elektroniką, dabar leidžia miniatiūrizuoti biologijos laboratorijas.
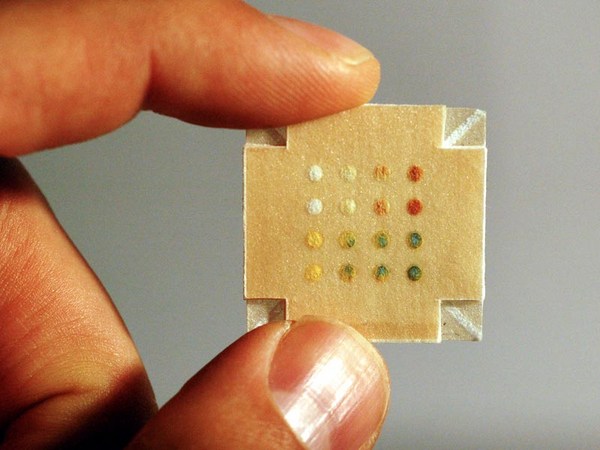
So, right now, we can actually miniaturize biological and chemistry laboratories onto microfluidic chips. I was very lucky to come to the US right after high school, and was able to work on this technology and develop some devices. This is a microfluidic chip that I developed. A close look at how the technology works: These are channels that are about the size of a human hair -- so you have integrated valves, pumps, mixers and injectors -- so you can fit entire diagnostic experiments onto a microfluidic system.
Taigi dabar mes iš tiesų galime miniatiūrizuoti biologijos ir chemijos laboratorijas ant mikrofluidinių mikroschemų. Man labai pasisekė atsirasti JT iškart po mokyklos ir dirbti prie šios technologijos ir išvystyti keletą prietaisų. Tai - mikrofliudinė mikroschema, kurią aš sukūriau. Arčiau pažiūrėjus kaip ši technologija veikia: čia yra kanalai storio sulig žmogaus plauku. Turime integruotus vožtuvus, siurblius, mikserius ir purkštuvus, taigi galime sumontuoti ištisus diagnostinius eksperimentus ant mikrofluidinės sistemos.
So what I plan to do with this technology is to actually take the current state of the technology and build an HIV kit in a microfluidic system. So, with one microfluidic chip, which is the size of an iPhone, you can actually diagnose 100 patients at the same time. For each patient, we will be able to do up to 100 different viral loads per patient. And this is only done in four hours, 50 times faster than the current state of the art, at a cost that will be five to 500 times cheaper than the current options. So this will allow us to create personalized medicines in the Third World at a cost that is actually achievable and make the world a safer place.
Aš planuoju pasinaudoti dabartine šios technologijos būsena ir mikrofluidinėje sistemoje pagaminti ŽIV rinkinį taip, kad su viena mikrofluidine mikroschema, kurios dydis būtų kaip iPhone, būtų galima diagnozuoti 100 pacientų vienu metu. Kiekvienam pacientui mes galėtume atlikti virš 100 skirtingų virusinių užtaisų per pacientą. Ir tai įmanoma padaryti per keturias valandas, 50 kartų greičiau nei dabar ir 5-500 kartų pigiau, nei dabar. Taigi, tai leis mums sukurti personalizuotus trečiojo pasaulio vaistus, kurių kaina bus prieinama, ir padėti pasauliui tapti saugesne vieta.
I invite your interest as well as your involvement in driving this vision to a point of practical reality.
Aš kviečiu Jus visus apgalvoti ir prisidėti prie šios vizijos plėtojimo siekiant visa tai paversti realybe.
Thank you very much.
Labai Jums ačiū.
(Applause)
(Plojimai)