The greatest irony in global health is that the poorest countries carry the largest disease burden. If we resize the countries of the globe in proportion to the subject of interest, we see that Sub-Saharan Africa is the worst hit region by HIV/AIDS. This is the most devastating epidemic of our time. We also see that this region has the least capability in terms of dealing with the disease. There are very few doctors and, quite frankly, these countries do not have the resources that are needed to cope with such epidemics.
전세계 보건에 관해 제일 역설적인 사실은 가장 가난한 국가들이 질병에 관해 가장 큰 부담을 지고 있는 것입니다. 전세계 국가들을 그 질병에 대한 이해관계에 비례해서 크기를 조정해 본다면, 사하라 사막 이남 아프리카 지역이 에이즈로 가장 큰 타격을 받는 것을 알 수 있습니다. 에이즈는 우리 시대 가장 심각한 전염병입니다. 또 이 지역은 이 질병에 대처할 수 있는 능력이 가장 떨어지는 곳이기도 합니다. 의사의 수가 너무 적고 솔직히 말해서 이 국가들은 이러한 전염병에 제대로 대처할 수 있는 자원이 부족합니다.
So what the Western countries, developed countries, have generously done is they have proposed to provide free drugs to all people in Third World countries who actually can't afford these medications. And this has already saved millions of lives, and it has prevented entire economies from capsizing in Sub-Saharan Africa.
그래서 서방 국가들과 선진국들이 실제 약을 살 능력이 없는 제3세계 국가 모든 이들에게 약을 무료로 공급하겠다는 선의의 제안을 하기도 했습니다. 이를 통해 이미 수백 만 명의 목숨을 구했고 또 사하라 사막 이남 국가들 경제 전체가 공멸하는 것을 막기도 했습니다.
But there is a fundamental problem that is killing the efforts in fighting this disease, because if you keep throwing drugs out at people who don't have diagnostic services, you end up creating a problem of drug resistance. This is already beginning to happen in Sub-Saharan Africa. The problem is that, what begins as a tragedy in the Third World could easily become a global problem. And the last thing we want to see is drug-resistant strains of HIV popping up all over the world, because it will make treatment more expensive and it could also restore the pre-ARV carnage of HIV/AIDS.
그러나, 아직 근본적인 문제가 존재하는데, 바로 그러한 도움들이 질병과 싸우고자 하는 노력을 사그라들게한다는 것입니다. 만약 질병에 대한 진단을 제대로 받을 수 없는 사람들에게 계속 약을 나눠주기만 한다면 결국 그 약에 대한 내성만 생기게 할 뿐입니다. 사하라 사막 이남 아프리카 지역에선 이미 이 일이 일어나고 있습니다. 문제는 제3세계의 비극으로 시작한 것이, 쉽게 전세계적인 문제가 될 수 있다는 것이고 가장 목격하기 두려운 건, 약제 내성을 가진 에이즈 병원체들이 전세계 곳곳에서 출현하는 것인데 그렇게 되면 치료는 더욱 비싸지고, 항바이러스제제가 없던 시절 에이즈가 초래했던 대규모 인명 희생이 재현될 수도 있습니다.
I experienced this firsthand as a high school student in Uganda. This was in the 90s during the peak of the HIV epidemic, before there were any ARVs in Sub-Saharan Africa. And during that time, I actually lost more relatives, as well as the teachers who taught me, to HIV/AIDS. So this became one of the driving passions of my life, to help find real solutions that could address these kinds of problems.
제가 우간다에서 고등학생일 때 이런 일을 실제로 경험했습니다. 1990년대 에이즈가 극심하게 창궐하고 사하라 사막 이남 아프리카 지역에서 아직 항바이러스제제가 나오기 전이었습니다. 그 시기에 실제로 저는 에이즈에 저를 가르쳐주신 선생님들 뿐 아니라 많은 친척들을 잃었습니다. 그래서 제 인생에서 열정을 다하는 일 중 하나가, 바로 이러한 문제들을 해결할 수 있는 실질적인 방법들을 찾는 것입니다.
We all know about the miracle of miniaturization. Back in the day, computers used to fill this entire room, and people actually used to work inside the computers. But what electronic miniaturization has done is that it has allowed people to shrink technology into a cell phone. And I'm sure everyone here enjoys cell phones that can actually be used in the remote areas of the world, in the Third World countries. The good news is that the same technology that allowed miniaturization of electronics is now allowing us to miniaturize biological laboratories.
소형화가 주는 놀라운 기적에 대해선 다들 알고 있습니다. 예전 컴퓨터들은 이 방 전체를 한가득 채울 정도로 컸고, 사람들은 실제로 컴퓨터 안에 들어가 일하기도 했습니다. 하지만 전자제품의 소형화를 통해 사람들은 기술집약을 이루어 냈고 결국 무선전화를 만들기에 이르렀습니다. 여기 있는 분들이 즐겨쓰시는 무선전화가 제3세계 국가, 어느 외지에서도 실제로 똑같이 사용되고 있을 겁니다. 한 가지 좋은 소식은 이와 같은 전자제품의 소형화를 이루어낸 바로 그 기술이 생물 실험실의 소형화를 가능케 한다는 겁니다.
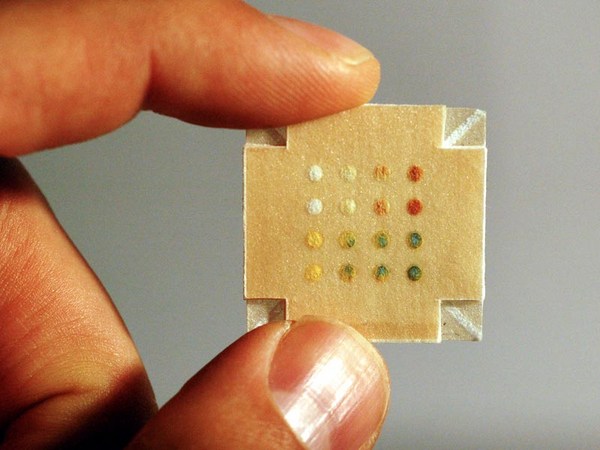
So, right now, we can actually miniaturize biological and chemistry laboratories onto microfluidic chips. I was very lucky to come to the US right after high school, and was able to work on this technology and develop some devices. This is a microfluidic chip that I developed. A close look at how the technology works: These are channels that are about the size of a human hair -- so you have integrated valves, pumps, mixers and injectors -- so you can fit entire diagnostic experiments onto a microfluidic system.
사실 지금도 당장 생물 화학 실험실들을 이 microfluidic(미세유체학) 칩 안으로 소형화 시킬 수 있습니다. 전 운이 좋아서 고등학교를 마치고 바로 미국에 건너와 이러한 기술에 대해 연구하고 몇몇 장치들을 개발할 수 있었습니다. 지금 보여드리는 것은 제가 개발한 미세유체학 칩입니다. 이 기술이 어떻게 작용하는지 자세히 보자면, 이것들은 사람 머리카락 크기 정도의 채널들입니다. 여기에 밸브, 펌프, 혼합기나 주입기들을 결합시켜 전체 진단실험들을 하나의 미세유체학 시스템에 꼭 맞춰 넣을 수 있습니다.
So what I plan to do with this technology is to actually take the current state of the technology and build an HIV kit in a microfluidic system. So, with one microfluidic chip, which is the size of an iPhone, you can actually diagnose 100 patients at the same time. For each patient, we will be able to do up to 100 different viral loads per patient. And this is only done in four hours, 50 times faster than the current state of the art, at a cost that will be five to 500 times cheaper than the current options. So this will allow us to create personalized medicines in the Third World at a cost that is actually achievable and make the world a safer place.
제가 이 기술을 가지고 계획하고 있는 것은 실제로 현재의 기술수준을 이용하여 하나의 미세유체학 시스템에 에이즈 진단키트를 만드는 겁니다. 그러면 아이폰 정도 크기의 미세유체학 칩 하나로 동시에 100명의 환자를 실제로 진단할 수 있습니다. 또 환자 한 명 당 백 가지 다른 바이러스에 대해 진단할 수 있습니다. 이것도 4시간 만에 끝나는데 현 수준에 비해 50배는 빠르고 5배에서 500배는 저렴하게 진단할 수 있습니다. 그렇게 하면 현실적으로 가능한 비용으로 제3세계에 맞춤형 의료 서비스를 제공할 수 있고 전세계를 더욱 안전한 곳으로 만들 수 있습니다.
I invite your interest as well as your involvement in driving this vision to a point of practical reality.
이러한 계획이 구체적으로 실현될 수 있도록, 여러분의 관심과 아울러 참여를 부탁드립니다.
Thank you very much.
고맙습니다.
(Applause)
(박수)