So I'm a doctor, but I kind of slipped sideways into research, and now I'm an epidemiologist. And nobody really knows what epidemiology is. Epidemiology is the science of how we know in the real world if something is good for you or bad for you. And it's best understood through example as the science of those crazy, wacky newspaper headlines. And these are just some of the examples.
Eu son médico, pero inclineime pola investigación e agora son epidemiólogo. E ninguén sabe de certo que é a epidemioloxía. A epidemioloxía é a ciencia que estuda como saber no mundo real se algo é bo ou malo para nós. Enténdese mellor a través dun exemplo: é a ciencia deses titulares tolos, absurdos, dos xornais. Imos ver algúns exemplos.
These are from the Daily Mail. Every country in the world has a newspaper like this. It has this bizarre, ongoing philosophical project of dividing all the inanimate objects in the world into the ones that either cause or prevent cancer. Here are some of the things they said cause cancer: divorce, Wi-Fi, toiletries and coffee. Some things they say prevent cancer: crusts, red pepper, licorice and coffee. So you can see there are contradictions. Coffee both causes and prevents cancer. As you start to read on, you can see that maybe there's some political valence behind some of this. For women, housework prevents breast cancer, but for men, shopping could make you impotent.
Este é do Daily Mail. Todos os países teñen un xornal coma este. Ten o estraño proxecto filosófico de dividir os obxectos inanimados do mundo nos que causan cancro e nos que o preveñen. Segundo eles, causan cancro: o divorcio, a rede sen fíos, os artigos de aseo e o café. E preveñen o cancro: a codia, o pemento vermello, a regalicia e o café. Como podedes ver, hai contradicións. O café causa cancro e á vez preveno. E cando comezades a ler vedes que quizais haxa algún tipo de interese político por tras. Para as mulleres, o traballo doméstico causa cancro de mama pero para os homes, comprar pode facelos impotentes.
(Laughter)
Así que hai que comezar
So we know that we need to start unpicking the science behind this. And what I hope to show is that unpicking the evidence behind dodgy claims isn't a kind of nasty, carping activity; it's socially useful. But it's also an extremely valuable explanatory tool, because real science is about critically appraising the evidence for somebody else's position. That's what happens in academic journals, it's what happens at academic conferences -- the Q&A session after a postdoc presents data is often a bloodbath. And nobody minds that; we actively welcome it. It's like a consenting intellectual S&M activity.
descifrando a ciencia que hai aí detrás. E espero demostrar que examinar afirmacións tan arriscadas, examinar a evidencia que subxace a elas non é rosmar con mala intención; socialmente é útil, pero ademais é unha ferramenta explicativa extremadamente valiosa. Porque a ciencia verdadeira consiste na avaliación crítica das probas que avalan unha postura. Así se fai nas publicacións académicas. E nas reunións académicas. As preguntas que seguen unha presentación de datos adoitan ser un baño de sangue. E a ninguén lle importa. Gústanos. É como unha actividade intelectual sadomasoquista consensuada.
(Laughter)
Así que vou amosarvos
So what I'm going to show you is all of the main things, all of the main features of my discipline, evidence-based medicine. And I will talk you through all of these and demonstrate how they work, exclusively using examples of people getting stuff wrong.
as partes principais, as características principais da miña disciplina: a medicina baseada en evidencias. Explicaréivolas e demostrareivos como funcionan usando exclusivamente exemplos de xente que o fai mal.
We'll start with the absolute weakest form of evidence known to man, and that is authority. In science, we don't care how many letters you have after your name -- we want to know what your reasons are for believing something. How do you know that something is good for us or bad for us? But we're also unimpressed by authority because it's so easy to contrive. This is somebody called Dr. Gillian McKeith, PhD, or, to give her full medical title, Gillian McKeith.
Así que comezaremos coa forma máis débil de evidencia coñecida polo home: a autoridade. Na ciencia, non nos importa cantos títulos tes. O que queremos é saber as túas razóns para crer en algo. Como sabes que algo é bo ou malo para nós? Non nos impresiona a autoridade, porque é tan fácil inventala... Esta é a Dra. Gillian McKeith ou, para darlle o seu título médico completo, Gillian McKeith.
(Laughter)
(Risos)
Again, every country has somebody like this. She is our TV diet guru. She has five series of prime-time television, giving out very lavish and exotic health advice. She, it turns out, has a non-accredited correspondence course PhD from somewhere in America. She also boasts that she's a certified professional member of the American Association of Nutritional Consultants, which sounds very glamorous; you get a certificate. This one belongs to my dead cat, Hettie. She was a horrible cat. You go to the website, fill out the form, give them $60, it arrives in the post. That's not the only reason we think this person is an idiot. She also says things like eat lots of dark green leaves, they contain chlorophyll and really oxygenate your blood. And anybody who's done school biology remembers that chlorophyll and chloroplasts only make oxygen in sunlight, and it's quite dark in your bowels after you've eaten spinach.
En fin, todos os países teñen alguén así. É a nosa gurú mediática das dietas. Ten cinco programas de televisión en horario de máxima audiencia nos que dá consellos moi exóticos sobre saúde. Resulta que ten un doutoramento non oficial por correspondencia, de algures nos Estados Unidos. Tamén se gaba de ser membro certificado da Asociación Americana de Consultores Nutricionais, que soa moi glamuroso e fascinante. Danche un certificado e todo. Este é de Hetti, a miña defunta gata. Unha gata horrible. Vas á web, enches o impreso, dáslles 60 dólares e chégache por correo. Pero esta non é a única razón para pensar que é idiota. Tamén vai e di cousas como que deberiamos comer moita verdura verde escura porque ten moita clorofila e iso osixena o sangue. Calquera que estudara bioloxía na escola lembra que a clorofila e os cloroplastos só producen osíxeno á luz do día e os intestinos están bastante escuros para as espinacas.
Next, we need proper science, proper evidence. So: "Red wine can help prevent breast cancer." This is a headline from The Daily Telegraph in the UK. "A glass of red wine a day could help prevent breast cancer." So you find this paper, and find that it is a real piece of science. It's a description of the changes in the behavior of one enzyme when you drip a chemical extracted from some red grape skin onto some cancer cells in a dish on a bench in a laboratory somewhere. And that's a really useful thing to describe in a scientific paper. But on the question of your own personal risk of getting breast cancer if you drink red wine, it tells you absolutely bugger all. Actually, it turns out that your risk of breast cancer increases slightly with every amount of alcohol you drink. So what we want are studies in real human people.
Seguimos. Precisamos ciencia e evidencia axeitadas. "O viño tinto axuda a previr o cancro de mama." Este é un titulardo Daily Telegraph do Reino Unido. "Un vaso de viño tinto ao día axuda a previr o cancro de mama." Pero collemos o xornal e descubrimos que é un verdadeiro artigo científico. É a descrición dos cambios nun enzima ao colocar unha gota dun produto químico extraído da tona da uva tinta en células cancerosas nunha mesa de laboratorio en algures. E esa é unha cousa moi útil para describir nunha publicación científica, pero en canto ao risco persoal de ter cancro de mama se bebemos viño tinto, non di nada. En realidade, resulta que o risco de cancro de mama aumenta un pouco canto máis alcol bebemos. Queremos estudos feitos en xente real.
And here's another example. This is from Britain's "leading" diet nutritionist in the Daily Mirror, our second-biggest selling newspaper. "An Australian study in 2001 found that olive oil, in combination with fruits, vegetables and pulses, offers measurable protection against skin wrinklings," and give the advice: "If you eat olive oil and vegetables, you'll have fewer wrinkles." They helpfully tell you how to find the paper, and what you find is an observational study. Obviously, nobody has been able to go back to 1930, get all the people born in one maternity unit, and half of them eat lots of fruit and veg and olive oil, half of them eat McDonald's, and then we see how many wrinkles you've got later.
Aquí hai outro exemplo do destacado nutricionista británico do Daily Mirror, o noso segundo xornal máis vendido: "Un estudo australiano do 2001 atopou que o aceite de oliva combinado con froitas, vexetais e legumes protexe contra as engurras da pel." E despois dános un consello: "Se tomamos aceite de oliva e vexetais teremos menos engurras." E dinos como atopar a publicación. Así que buscas o artigo e o que atopas é un estudo observacional. Obviamente, ninguén puido ir a 1930, coller os bebés dunha maternidade, facer que a metade comese moita froita, verduras e aceite de oliva e a que outra metade comese McDonald's e despois analizar as súas engurras.
You have to take a snapshot of how people are now. And what you find is, of course: people who eat veg and olive oil have fewer wrinkles. But that's because people who eat fruit and veg and olive oil are freaks -- they're not normal, they're like you; they come to events like this.
Hai que facer unha mostraxe de como son as persoas agora. E o que atopas, claro, é que a xente que come verduras e aceite de oliva ten menos engurras. Pero iso é porque a xente que come froita e aceite de oliva é rara, non é normal, é coma vós; veñen a eventos coma este.
(Laughter)
Son elegantes, son ricos, traballan menos ao aire libre,
They're posh, they're wealthy, less likely to have outdoor jobs, less likely to do manual labor, they have better social support, are less likely to smoke; for a host of fascinating, interlocking social, political and cultural reasons, they're less likely to have wrinkles. That doesn't mean it's the vegetables or olive oil.
fan menos traballos manuais, teñen máis apoio social, fuman menos... así que por unha chea de fascinantes razóns, sociais, políticas e culturais entrelazadas, é menos probable que teñan engurras na pel. Iso non significa que sexa polos vexetais e o aceite de oliva.
(Laughter)
(Risos)
So ideally, what you want to do is a trial. People think they're familiar with the idea of a trial. Trials are old; the first one was in the Bible, Daniel 1:12. It's straightforward: take a bunch of people, split them in half, treat one group one way, the other group, the other way. A while later, you see what happened to each of them. I'm going to tell you about one trial, which is probably the most well-reported trial in the UK news media over the past decade. This is the trial of fish oil pills. The claim: fish oil pills improve school performance and behavior in mainstream children. They said, "We did a trial. All the previous ones were positive, this one will be too." That should ring alarm bells: if you know the answer to your trial, you shouldn't be doing one. Either you've rigged it by design, or you've got enough data so there's no need to randomize people anymore.
Entón, o ideal sería facer un ensaio. Todo o mundo cre que sabe que é un ensaio. Os ensaios son moi antigos. O primeiro está na Biblia, Daniel 1:12. É moi fácil, cóllese un grupo de xente, divídese en dous, trátase un grupo dun xeito, e o outro, doutro, e despois, fáiselles un seguimento para ver que ocorre con cada un. Así que vou falarvos dun ensaio que foi probablemente o máis popular nos medios británicos na pasada década. É o ensaio das pílulas de aceite de peixe. Dicíase que melloraban o rendemento escolar e o comportamento na maioría dos nenos. Dixeron: "Fixemos un ensaio. Os anteriores foron positivos e sabemos que este tamén." Iso sempre debería facer soar unha alarma. Porque se xa se sabe a resposta do ensaio non se debería facer. Ou está manipulado o deseño ou xa hai datos dabondo, así que non é preciso probalo en máis persoas.
So this is what they were going to do in their trial: They were taking 3,000 children, they were going to give them these huge fish oil pills, six of them a day, and then, a year later, measure their school exam performance and compare their performance against what they predicted their exam performance would have been if they hadn't had the pills. Now, can anybody spot a flaw in this design?
Isto é o que ían facer no seu ensaio. Ían coller 3 000 nenos, ían darlles unhas enormes pílulas de aceite de peixe, seis ao día, e un ano máis tarde, ían medir o rendemento escolar en exames e comparar ese rendemento co que eles calculaban que terían se non tomaran as pílulas. Pode ver alguén o punto fraco no deseño?
(Laughter)
Se sodes profesores de metodoloxía de ensaios clínicos
And no professors of clinical trial methodology are allowed to answer this question. So there's no control group. But that sounds really techie, right? That's a technical term. The kids got the pills, and their performance improved.
non respondades esta cuestión. Non hai control; non hai ningún grupo de control. Pero isto soa moi técnico. É un termo técnico. Os rapaces tomaron as pílulas e o seu rendemento mellorou.
What else could it possibly be if it wasn't the pills? They got older; we all develop over time. And of course, there's the placebo effect, one of the most fascinating things in the whole of medicine. It's not just taking a pill and performance or pain improving; it's about our beliefs and expectations, the cultural meaning of a treatment. And this has been demonstrated in a whole raft of fascinating studies comparing one kind of placebo against another. So we know, for example, that two sugar pills a day are a more effective treatment for gastric ulcers than one sugar pill. Two sugar pills a day beats one a day. That's an outrageous and ridiculous finding, but it's true. We know from three different studies on three different types of pain that a saltwater injection is a more effective treatment than a sugar pill, a dummy pill with no medicine in it, not because the injection or pills do anything physically to the body, but because an injection feels like a much more dramatic intervention. So we know that our beliefs and expectations can be manipulated, which is why we do trials where we control against a placebo, where one half of the people get the real treatment, and the other half get placebo.
Que outra cousa podería ser senón as pílulas? Medraron. Todos evolucionamos co tempo. Por suposto, tamén está o efecto placebo, que é unha das cousas máis fascinantes en medicina. E non se trata só de tomar unha pílula e que mellore o rendemento e a dor. Trátase das nosas crenzas e expectativas. Do significado cultural dun tratamento. E isto demostrouse nunha chea de estudos fascinantes que comparaban un tipo de placebo con outro. Sabemos, por exemplo, que 2 pílulas de azucre ao día son máis efectivas para as úlceras gástricas que unha soa pílula de azucre. 2 pílulas ao día son mellores que unha. Ese é un achado estraño e ridículo, pero verdadeiro. Sabemos por 3 estudos diferentes sobre 3 tipos de dor que unha inxección de auga salgada é máis efectivo para a dor que tomar unha pílula de azucre, unha pílula que non contén nada, non porque unha nin outra fagan algo fisicamente no corpo, senón porque a inxección parece unha intervención máis drástica. Sabemos que as nosas crenzas e expectativas poden ser manipuladas, por iso facemos ensaios onde comparamos un control cun un placebo: a metade da xente recibe o tratamento real e a outra metade, o placebo.
But that's not enough. What I've just shown you are examples of the very simple and straightforward ways that journalists and food supplement pill peddlers and naturopaths can distort evidence for their own purposes. What I find really fascinating is that the pharmaceutical industry uses exactly the same kinds of tricks and devices, but slightly more sophisticated versions of them, in order to distort the evidence they give to doctors and patients, and which we use to make vitally important decisions.
Pero non abonda. O que vos amosei son exemplos das formas sinxelas e directas en que xornalistas e vendedores de suplementos dietéticos e naturópatas terxiversan as probas a favor dos seus propios intereses. O que é realmente fascinante é que a industria farmacéutica usa exactamente os mesmos trucos e instrumentos pero con versións lixeiramente máis sofisticadas para terxiversar as probas que lles dan a médicos e pacientes e que usamos para tomar decisións vitais.
So firstly, trials against placebo: everybody thinks a trial should be a comparison of your new drug against placebo. But in a lot of situations that's wrong; often, we already have a good treatment currently available. So we don't want to know that your alternative new treatment is better than nothing, but that it's better than the best available treatment we have. And yet, repeatedly, you consistently see people doing trials still against placebo. And you can get licensed to bring your drug to market with only data showing that it's better than nothing, which is useless for a doctor like me trying to make a decision.
En primeiro lugar, o ensaio con placebos: todo o mundo pensa que un ensaio debería ser unha comparación entre un novo fármaco e un placebo. Pero, realmente, moitas veces non é así porque a miúdo xa existe un bo tratamento así que non queremos saber se o novo tratamento alternativo é mellor que nada. Queremos saber se supera o mellor dos tratamentos que xa temos. E aínda así, de xeito repetido vemos xente que fai ensaios contra o placebo. E pódese obter licenza para sacar un fármaco ao mercado só cuns datos que digan que é mellor que nada, algo inútil para un médico coma min que intenta tomar unha decisión.
But that's not the only way you can rig your data. You can also rig your data by making the thing you compare your new drug against really rubbish. You can give the competing drug in too low a dose, so people aren't properly treated. You can give the competing drug in too high a dose, so people get side effects. And this is exactly what happened with antipsychotic medication for schizophrenia. Twenty years ago, a new generation of antipsychotic drugs were brought in; the promise was they would have fewer side effects. So people set about doing trials of the new drugs against the old drugs. But they gave the old drugs in ridiculously high doses: 20 milligrams a day of haloperidol. And it's a foregone conclusion if you give a drug at that high a dose, it will have more side effects, and your new drug will look better.
Pero non é a única forma de manipular os datos. Tamén pode facerse comparando o novo fármaco con algo inútil. Pódese dar o fármaco competidor en dose moi baixa para que a xente non teña o tratamento adecuado. Ou nunha dose moi alta para que produza efectos secundarios. Isto foi talmente o que ocorreu cos antipsicóticos para a esquizofrenia. Hai 20 anos, apareceu unha nova xeración de antipsicóticos coa promesa de que terían menos efectos secundarios. Así que se comezaron a facer ensaios con eles comparándoos cos vellos pero dábanse doses ridiculamente altas dos vellos fármacos -20 mg ao día de haloperidol. E é unha conclusión evidente que se se dá un fármaco nunha dose tan alta terá máis efectos secundarios e o novo parecerá mellor.
Ten years ago, history repeated itself, when risperidone, the first of the new-generation antipsychotic drugs, came off copyright, so anybody could make copies. Everybody wanted to show their drug was better than risperidone, so you see trials comparing new antipsychotic drugs against risperidone at eight milligrams a day. Again, not an insane dose, not an illegal dose, but very much at the high end of normal. So you're bound to make your new drug look better. And so it's no surprise that overall, industry-funded trials are four times more likely to give a positive result than independently sponsored trials.
Hai 10 anos, repetiuse a historia cando a risperidona, o primeiro antipsicótico da nova xeración, xa non tiña dereitos de autor, e podía reproducirse libremente. Todos querían probar que o seu fármaco era mellor ca ela así que houbo moitos ensaios que comparaban os novos antipsicóticos con 8 mg por día de risperidona. Outra vez, non é unha dose absurda, non é ilegal, pero está moi cerca de superar o normal. Así, seguro que o novo fármaco parecerá mellor. Polo tanto, non sorprende que, en xeral, os ensaios financiados pola industria teñan 4 veces máis probabilidades de dar un resultado positivo que os independentes.
But -- and it's a big but --
Pero -e este é un pero moi grande-
(Laughter)
(Risos)
it turns out, when you look at the methods used by industry-funded trials, that they're actually better than independently sponsored trials. And yet, they always manage to get the result that they want. So how does this work?
resulta que cando observas os métodos usados en ensaios financiados pola industria ves que son realmente mellores que os independentes. E, aínda así, sempre conseguen os resultados que queren. Entón..., como pode ser?
(Laughter)
(Risos)
How can we explain this strange phenomenon? Well, it turns out that what happens is the negative data goes missing in action; it's withheld from doctors and patients. And this is the most important aspect of the whole story. It's at the top of the pyramid of evidence. We need to have all of the data on a particular treatment to know whether or not it really is effective. There are two different ways you can spot whether some data has gone missing. You can use statistics or you can use stories. I prefer statistics, so that's what I'll do first.
Como podemos explicar este estraño fenómeno? Ben, pois o que ocorre é que os datos negativos pérdense en combate; non se revelan a médicos e pacientes. Este é o aspecto máis importante da historia. Está no cume da pirámide de probas. Precisamos ter todos os datos dun tratamento en concreto para saber se é efectivo ou non. E hai dous modos de ver se algúns datos se perderon en combate. Pódense usar estatísticas ou historias. Eu prefiro as estatísticas, así que empezarei por elas.
This is a funnel plot. A funnel plot is a very clever way of spotting if small negative trials have disappeared, have gone missing in action. This is a graph of all of the trials done on a particular treatment. As you go up towards the top of the graph, what you see is each dot is a trial. As you go up, those are bigger trials, so they've got less error; they're less likely to be randomly false positives or negatives. So they all cluster together. The big trials are closer to the true answer. Then as you go further down at the bottom, what you can see is, on this side, spurious false negatives, and over on this side, spurious false positives. If there is publication bias, if small negative trials have gone missing in action, you can see it on one of these graphs. So you see here that the small negative trials that should be on the bottom left have disappeared. This is a graph demonstrating the presence of publication bias in studies of publication bias. And I think that's the funniest epidemiology joke you will ever hear.
Isto é unha gráfica de funil. É unha moi boa forma de identificar se pequenos ensaios negativos desapareceron en combate. Esta é unha gráfica de todas as probas que se fixeron dun tratamento concreto. Ao observar a parte superior da gráfica vese que cada punto é un ensaio. E ao subir, estes son os ensaios máis grandes, con menos erros. É menos probable que dean falsos positivos ou falsos negativos. Así que todos se agrupan. Os grandes ensaios están máis cerca da resposta real. Cando imos cara ao fondo, o que vemos é, neste lado, os falsos negativos espurios e, neste lado, os falsos positivos espurios. Se hai un nesgo na publicación se os pequenos ensaios negativos desapareceron, pódese ver nunha destas gráficas. Aquí pódese ver que os pequenos ensaios negativos que deberían estar abaixo á esquerda desapareceron. Esta gráfica demostra a presenza de nesgos na publicación en estudos sobre nesgos nas publicacións. E penso que esta é a broma epidemiolóxica
(Laughter)
máis graciosa que escoitastes.
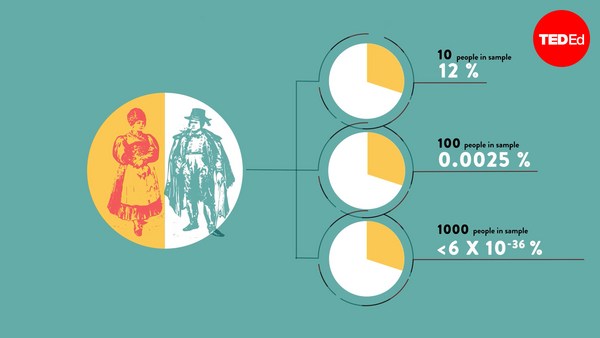
That's how you can prove it statistically. But what about stories? Well, they're heinous, they really are. This is a drug called reboxetine. This is a drug which I, myself, have prescribed to patients. And I'm a very nerdy doctor. I hope I go out of my way to try and read and understand all the literature. I read the trials on this. They were all positive, all well-conducted. I found no flaw. Unfortunately, it turned out, that many of these trials were withheld. In fact, 76 percent of all of the trials that were done on this drug were withheld from doctors and patients. Now if you think about it, if I tossed a coin a hundred times, and I'm allowed to withhold from you the answers half the times, then I can convince you that I have a coin with two heads. If we remove half of the data, we can never know what the true effect size of these medicines is.
Así é como se proba estatisticamente, pero que pasa coas historias? Ben, son odiosas, abofé que si. Hai un fármaco chamado reboxetina. É un medicamento que eu mesmo lles prescribín a pacientes. E son un médico moi aplicado. Fago o posible por intentar ler e entender a bibliografía. Lin os ensaios sobre este fármaco. Todos positivos. Todos ben dirixidos. Non atopei puntos febles. Por desgraza, resultou que moitos deses ensaios, en realidade, o 76 % dos que se fixeron con este fármaco ocultáronselles a médicos e pacientes. Se o pensades, se eu tiro unha moeda ao ar cen veces, e se me permite ocultar o resultado a metade das veces, podería convencervos de que teño unha moeda de dúas caras. Se eliminamos a metade dos datos, nunca poderemos saber os verdadeiros efectos dese fármaco.
And this is not an isolated story. Around half of all of the trial data on antidepressants has been withheld, but it goes way beyond that. The Nordic Cochrane Group were trying to get ahold of the data on that to bring it all together. The Cochrane Groups are an international nonprofit collaboration that produce systematic reviews of all of the data that has ever been shown. And they need to have access to all of the trial data. But the companies withheld that data from them. So did the European Medicines Agency -- for three years.
E isto non é unha historia illada. Case a metade da información de ensaios con antidepresivos está oculta pero isto vai máis alá. O Nordic Cochrane Group intentou acceder a esa información para agrupala. Os Cochrane Groups son unha alianza internacional sen fin de lucro que fai revisións sistemáticas de todos os datos que aparecen. E precisan ter acceso a todos os datos dos ensaios. Pero as compañías ocúltanlles esta información, tal como fixo tamén a Axencia Europea de Medicamentos durante 3 anos. Este é un problema actualmente sen solución.
This is a problem that is currently lacking a solution. And to show how big it goes, this is a drug called Tamiflu, which governments around the world have spent billions and billions of dollars on. And they spend that money on the promise that this is a drug which will reduce the rate of complications with flu. We already have the data showing it reduces the duration of your flu by a few hours. But I don't care about that, governments don't care. I'm sorry if you have the flu, I know it's horrible, but we're not going to spend billions of dollars trying to reduce the duration of your flu symptoms by half a day. We prescribe these drugs. We stockpile them for emergencies on the understanding they'll reduce the number of complications, which means pneumonia and death. The infectious diseases Cochrane Group, which are based in Italy, has been trying to get the full data in a usable form out of the drug companies, so they can make a full decision about whether this drug is effective or not, and they've not been able to get that information. This is undoubtedly the single biggest ethical problem facing medicine today. We cannot make decisions in the absence of all of the information.
E para amosarvos o seu tamaño, velaquí un fármaco chamado Tamiflu, en que os gobernos do mundo gastaron miles e miles de millóns de dólares. E gastáronos coa promesa de que era un fármaco que reduciría a taxa de complicacións da gripe. Xa temos os datos que din que reduce a duración da gripe nunhas horas. Pero a min éme igual. E aos gobernos tamén. Sinto que teñades a gripe, sei que é horrible, pero non imos gastar miles de millóns de dólares para intentar reducir a duración dos síntomas da túa gripe en medio día. Prescribimos eses fármacos, acumulámolos para emerxencias pensando que reducirían o número de complicacións, é dicir, pneumonía e morte. O Cochrane Group de enfermidades infecciosas, con sede en Italia, intentou obter das compañías farmacéuticas todos os datos nun formato usable para poder decidir de forma concluínte se o fármaco é efectivo ou non e non foron capaces de conseguir esa información. Este é, sen dúbida, o problema ético máis grande con que bate a medicina hoxe en día. Non podemos tomar decisións ao non termos toda a información.
So it's a little bit difficult from there to spin in some kind of positive conclusion. But I would say this: I think that sunlight is the best disinfectant. All of these things are happening in plain sight, and they're all protected by a force field of tediousness. And I think, with all of the problems in science, one of the best things that we can do is to lift up the lid, finger around at the mechanics and peer in.
Así que é un pouco difícil extraer algún tipo de conclusión positiva. Pero eu diría isto: creo que a luz do sol é o mellor desinfectante. Todas estas cousas están ocorrendo diante dos nosos ollos, e todas están protexidas por un campo de forza de tedio. E penso que, con todos os problemas da ciencia, unha das mellores cousas que podemos facer é levantar a tapa, remexer nos mecanismos e osmar.
Thank you very much.
Moitas grazas.
(Applause)
(Aplausos)