De fet sóc metge, però vaig desviar-me cap a la recerca, i ara sóc epidemiòleg. I ningú sap què és realment l'epidemiologia. L'epidemiologia és la ciència sobre com sabem en el món real si una cosa és bona o dolenta per a tu. S'entén millor amb exemples, com ara la ciència d'aquests titulars estrafolaris dels diaris. I aquests són només alguns exemples.
So I'm a doctor, but I kind of slipped sideways into research, and now I'm an epidemiologist. And nobody really knows what epidemiology is. Epidemiology is the science of how we know in the real world if something is good for you or bad for you. And it's best understood through example as the science of those crazy, wacky newspaper headlines. And these are just some of the examples.
Aquest és del Daily Mail. Tots els països del món tenen un diari similar a aquest. Estan duent a terme un estrany projecte filosòfic de dividir tots els objectes inanimats del món en coses que causen o prevenen el càncer. Segons ells, causen càncer: el divorci, el Wi-Fi, els articles de tocador i el cafè. I, segons ells, prevenen el càncer: la crosta de pa, el pebrot vermell, la regalèssia i el cafè. Com podeu veure, hi ha contradiccions. El cafè tant causa com prevé el càncer. I quan segueixes llegint, veus que potser hi ha algun interès polític al darrere d'això. En les dones, les feines de casa prevenen el càncer, però en els homes, anar de compres pot causar impotència. Així sabem que necessitem començar
These are from the Daily Mail. Every country in the world has a newspaper like this. It has this bizarre, ongoing philosophical project of dividing all the inanimate objects in the world into the ones that either cause or prevent cancer. Here are some of the things they said cause cancer: divorce, Wi-Fi, toiletries and coffee. Some things they say prevent cancer: crusts, red pepper, licorice and coffee. So you can see there are contradictions. Coffee both causes and prevents cancer. As you start to read on, you can see that maybe there's some political valence behind some of this. For women, housework prevents breast cancer, but for men, shopping could make you impotent.
a examinar la ciència que hi ha darrere.
(Laughter) So we know that we need to start unpicking the science behind this.
I espero demostrar que examinar aquestes afirmacions dubtoses, examinar l'evidència darrere aquestes afirmacions dubtoses, no és una activitat criticaire malintencionada; és socialment útil, i també és una eina explicativa extremadament valuosa. Perquè la ciència real consisteix a avaluar les dades en què es basa algú altre de manera crítica. Això és el que es fa en els diaris acadèmics. Això és el que es fa en les conferències acadèmiques. La tanda de preguntes en acabar una presentació de dades sovint és un bany de sang. I a ningú li molesta. De fet, ens agrada. És com una activitat intel·lectual sadomasoquista consentida. Ara us ensenyaré tot el principal, les característiques principals de la meva disciplina: la medicina basada en l'evidència. Us les explicaré totes i us demostraré com funcionen utilitzant exclusivament exemples de gent que s'ha equivocat.
And what I hope to show is that unpicking the evidence behind dodgy claims isn't a kind of nasty, carping activity; it's socially useful. But it's also an extremely valuable explanatory tool, because real science is about critically appraising the evidence for somebody else's position. That's what happens in academic journals, it's what happens at academic conferences -- the Q&A session after a postdoc presents data is often a bloodbath. And nobody minds that; we actively welcome it. It's like a consenting intellectual S&M activity. (Laughter) So what I'm going to show you is all of the main things, all of the main features of my discipline, evidence-based medicine. And I will talk you through all of these and demonstrate how they work, exclusively using examples of people getting stuff wrong.
Començarem amb la forma més dèbil d'evidència coneguda per l'home: l'autoritat. En la ciència, no ens importa quants títols tens. En la ciència, volem saber quines raons tens per creure alguna cosa. Com saps si una cosa és bona per a nosaltres o si és dolenta? Però tampoc ens impressiona l'autoritat, perquè és fàcil de fingir. Aquí tenim algú anomenat Dra. Gillian McKeith, o, per donar-li el seu títol mèdic real, Gillian McKeith. (Rialles) De nou, tots els països tenen algú així. És la nostra guru de dietes televisiva. Té cinc programes en horari de màxima audiència, on dóna els seus consells de salut pròdigs i exòtics. Resulta que té un curs de doctorat per correspondència no acreditat d'algun lloc dels Estats Units. També presumeix de ser membre professional certificat de l'Associació Americana d'Assessors Nutricionals, que sona molt glamurós i excitant. Fins i tot et donen un certificat. Aquest és el de la meva difunta gata Hetti. Era una gata horrible. Senzillament entres a la web, omples el formulari, pagues 60 dòlars i t'arriba per correu. Però aquesta no és l'única raó per la qual pensem que és idiota. També perquè diu coses com: "Hauríeu de menjar moltes fulles verd fosc, perquè contenen molta clorofil·la i oxigenaran la vostra sang". Qualsevol que hagi fet biologia a l'escola recordarà que la clorofil·la i els cloroplasts només produeixen oxigen amb llum solar, i és bastant fosc en els teus intestins quan menges espinacs.
We'll start with the absolute weakest form of evidence known to man, and that is authority. In science, we don't care how many letters you have after your name -- we want to know what your reasons are for believing something. How do you know that something is good for us or bad for us? But we're also unimpressed by authority because it's so easy to contrive. This is somebody called Dr. Gillian McKeith, PhD, or, to give her full medical title, Gillian McKeith. (Laughter) Again, every country has somebody like this. She is our TV diet guru. She has five series of prime-time television, giving out very lavish and exotic health advice. She, it turns out, has a non-accredited correspondence course PhD from somewhere in America. She also boasts that she's a certified professional member of the American Association of Nutritional Consultants, which sounds very glamorous; you get a certificate. This one belongs to my dead cat, Hettie. She was a horrible cat. You go to the website, fill out the form, give them $60, it arrives in the post. That's not the only reason we think this person is an idiot. She also says things like eat lots of dark green leaves, they contain chlorophyll and really oxygenate your blood. And anybody who's done school biology remembers that chlorophyll and chloroplasts only make oxygen in sunlight, and it's quite dark in your bowels after you've eaten spinach.
A més, necessitem ciència com cal, evidència com cal. Per exemple: "El vi negre ajuda a prevenir el càncer de pit." Aquest és un titular del Daily Telegraph del Regne Unit: "Un got de vi negre diari pot ajudar a prevenir el càncer de pit." Així que agafes aquest diari, i hi trobes un article de ciència real. És la descripció dels canvis en un enzim quan degoteges un producte químic extret de la pell del raïm negre en unes cèl·lules cancerígenes en un plat en una taula de laboratori en algun lloc. Això és un fet realment útil de descriure en un article científic, però pel que fa al teu risc personal de tenir càncer de pit si beus vi negre, no et diu res de res. De fet, resulta que el risc de tenir càncer de pit s'incrementa lleugerament amb la quantitat d'alcohol que ingereixes. Així que el que cal son estudis en gent real.
Next, we need proper science, proper evidence. So: "Red wine can help prevent breast cancer." This is a headline from The Daily Telegraph in the UK. "A glass of red wine a day could help prevent breast cancer." So you find this paper, and find that it is a real piece of science. It's a description of the changes in the behavior of one enzyme when you drip a chemical extracted from some red grape skin onto some cancer cells in a dish on a bench in a laboratory somewhere. And that's a really useful thing to describe in a scientific paper. But on the question of your own personal risk of getting breast cancer if you drink red wine, it tells you absolutely bugger all. Actually, it turns out that your risk of breast cancer increases slightly with every amount of alcohol you drink. So what we want are studies in real human people.
Aquí teniu un altre exemple. Això és del dietista i nutricionista en cap del diari Daily Mirror, que és el segon diari en nombre de vendes al Regne Unit. "Un estudi australià del 2001 va descobrir que l'oli d'oliva combinat amb fruites, verdures i llegums secs ofereix una protecció apreciable contra les arrugues de la pell." I aleshores t'aconsellen: "Si menges oli d'oliva i verdures, tindràs menys arrugues a la pell." I t'ajuden dient on trobar aquest article. Així que busques l'article, i el que trobes és un estudi observacional. Evidentment ningú ha pogut tornar al 1930, agafar tota la gent nascuda en una unitat de maternitat, i que la meitat mengessin molta fruita, verdures i oli d'oliva, i que l'altra meitat mengés al McDonald's, i aleshores veuríem quantes arrugues acaben tenint.
And here's another example. This is from Britain's "leading" diet nutritionist in the Daily Mirror, our second-biggest selling newspaper. "An Australian study in 2001 found that olive oil, in combination with fruits, vegetables and pulses, offers measurable protection against skin wrinklings," and give the advice: "If you eat olive oil and vegetables, you'll have fewer wrinkles." They helpfully tell you how to find the paper, and what you find is an observational study. Obviously, nobody has been able to go back to 1930, get all the people born in one maternity unit, and half of them eat lots of fruit and veg and olive oil, half of them eat McDonald's, and then we see how many wrinkles you've got later.
Has de basar-te en dades de com és la gent ara. I el que trobes, evidentment, és que la gent que menja vegetals i oli d'oliva tenen menys arrugues. Però això és perquè la gent que menja fruites, vegetals i oli d'oliva són rarets, no són normals, són com vosaltres; vénen a actes com aquests. Són elegants, són rics, és menys probable que treballin a l'aire lliure, menys probable que facin treball manual, tenen un suport social millor, és menys probable que fumin, així que per un nombre enorme de raons fascinants, socials, polítiques i culturals, és menys probable que tinguin arrugues. Això no vol dir que sigui a causa de les verdures o l'oli d'oliva.
You have to take a snapshot of how people are now. And what you find is, of course: people who eat veg and olive oil have fewer wrinkles. But that's because people who eat fruit and veg and olive oil are freaks -- they're not normal, they're like you; they come to events like this. (Laughter) They're posh, they're wealthy, less likely to have outdoor jobs, less likely to do manual labor, they have better social support, are less likely to smoke; for a host of fascinating, interlocking social, political and cultural reasons, they're less likely to have wrinkles.
(Rialles)
That doesn't mean it's the vegetables or olive oil.
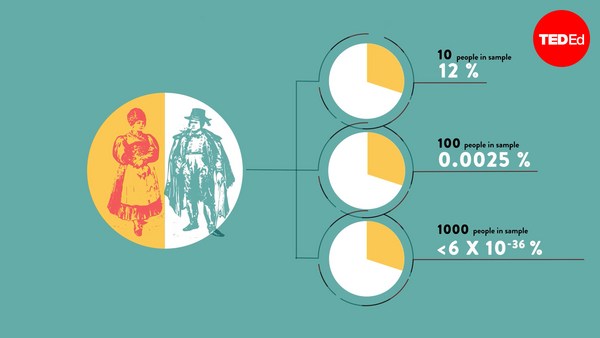
Així que l'ideal seria fer una prova. I tothom pensa que coneix bé en què consisteix una prova. Les proves són molt antigues. La primera està a la Bíblia, a Daniel 1:12. És molt fàcil: agafes un munt de gent, la divideixes per la meitat, tractes un grup d'una manera, i tractes l'altre grup d'una altra manera, i una mica després, els fas un seguiment i veus què els ha passat a cadascun d'ells. Us explicaré una prova, que segurament ha sigut la més ben seguida per tots els mitjans del Regne Unit en la última dècada. I és la prova de les píndoles d'oli de peix. Deien que les píndoles d'oli de peix milloren els resultats escolars i el comportament en la majoria de nens. Van dir: "Hem fet una prova. Les proves anteriors han estat positives, i sabem que aquesta també ho serà". Això sempre hauria de fer sonar l'alarma. Perquè si ja saps el resultat d'una prova, no l'hauries de fer. O bé l'has manipulat en dissenyar-la, o és que ja tens prou dades com per a no fer falta provar-ho en més gent.
(Laughter) So ideally, what you want to do is a trial. People think they're familiar with the idea of a trial. Trials are old; the first one was in the Bible, Daniel 1:12. It's straightforward: take a bunch of people, split them in half, treat one group one way, the other group, the other way. A while later, you see what happened to each of them. I'm going to tell you about one trial, which is probably the most well-reported trial in the UK news media over the past decade. This is the trial of fish oil pills. The claim: fish oil pills improve school performance and behavior in mainstream children. They said, "We did a trial. All the previous ones were positive, this one will be too." That should ring alarm bells: if you know the answer to your trial, you shouldn't be doing one. Either you've rigged it by design,
Això és el que farien en la seva prova. Agafarien 3.000 nens, els donarien totes aquestes píndoles enormes d'oli de peix, sis per dia, i, un any després, mesurarien els resultats dels seus exàmens escolars i compararien els resultats dels exàmens amb els resultats que ells havien previst que obtindrien si no haguessin pres les píndoles. Algú pot veure l'error en el seu disseny? I si sou professors de metodologia d'assaigs clínics no contesteu la pregunta. Doncs que no hi ha cap control; no hi ha grup de control. Però això sona massa científic. És un terme tècnic. Els nens van prendre les píndoles, i els seus resultats van millorar.
or you've got enough data so there's no need to randomize people anymore. So this is what they were going to do in their trial: They were taking 3,000 children, they were going to give them these huge fish oil pills, six of them a day, and then, a year later, measure their school exam performance and compare their performance against what they predicted their exam performance would have been if they hadn't had the pills. Now, can anybody spot a flaw in this design? (Laughter) And no professors of clinical trial methodology are allowed to answer this question. So there's no control group. But that sounds really techie, right? That's a technical term. The kids got the pills, and their performance improved.
Què més podria ser, excepte les píndoles? Es van fer grans. Tots ens anem desenvolupant. Per descomptat, també hi ha l'efecte placebo. L'efecte placebo és una de les coses més fascinants de tota la medicina. No és només que, per prendre una píndola, millori el teu estat o els teus resultats. Es tracta de les nostres creences i expectatives. Es tracta del significat cultural d'un tractament. I això s'ha demostrat en un munt d'estudis fascinants que comparen un tipus de placebo amb un altre. Sabem, per exemple, que dues píndoles de sucre al dia són un tractament més efectiu per lliurar-se de les úlceres gàstriques que una píndola de sucre. Dues píndoles de sucre al dia són millors que una píndola. És una troballa indignant i ridícula, però certa. Sabem per tres estudis diferents en tres tipus de dolor diferent que una injecció d'aigua salada és més efectiva per tractar el dolor que una píndola de sucre, una píndola de mentida sense cap medicament, no perquè la injecció o les píndoles facin res físicament al cos, sinó perquè una injecció sembla una intervenció molt més dràstica. Sabem que les nostres creences i expectatives poden ser manipulades, i és per això que fem proves on comparem amb un placebo, on a la meitat de gent se'ls dóna un tractament real i a l'altra meitat els donen un placebo.
What else could it possibly be if it wasn't the pills? They got older; we all develop over time. And of course, there's the placebo effect, one of the most fascinating things in the whole of medicine. It's not just taking a pill and performance or pain improving; it's about our beliefs and expectations, the cultural meaning of a treatment. And this has been demonstrated in a whole raft of fascinating studies comparing one kind of placebo against another. So we know, for example, that two sugar pills a day are a more effective treatment for gastric ulcers than one sugar pill. Two sugar pills a day beats one a day. That's an outrageous and ridiculous finding, but it's true. We know from three different studies on three different types of pain that a saltwater injection is a more effective treatment than a sugar pill, a dummy pill with no medicine in it, not because the injection or pills do anything physically to the body, but because an injection feels like a much more dramatic intervention. So we know that our beliefs and expectations can be manipulated, which is why we do trials where we control against a placebo, where one half of the people get the real treatment, and the other half get placebo.
Però no n'hi ha prou amb això. El que us he ensenyat són exemples de les maneres tan senzilles i directes en què periodistes, venedors de píndoles suplementàries i naturòpates poden distorsionar les dades pels seus propòsits. El que em sembla més fascinant és que la indústria farmacèutica utilitza exactament el mateix tipus de trucs i enganys, però amb versions una mica més sofisticades, per tal de distorsionar les dades que donen a doctors i pacients, i que nosaltres utilitzem per prendre decisions vitals.
But that's not enough. What I've just shown you are examples of the very simple and straightforward ways that journalists and food supplement pill peddlers and naturopaths can distort evidence for their own purposes. What I find really fascinating is that the pharmaceutical industry uses exactly the same kinds of tricks and devices, but slightly more sophisticated versions of them, in order to distort the evidence they give to doctors and patients, and which we use to make vitally important decisions.
Primer, proves contra un placebo: tothom creu que una prova hauria de ser una comparació del teu nou medicament amb un placebo. Però, de fet, en molt casos això no és cert. Perquè, sovint, ja disposem d'un bon tractament disponible, així que no ens interessa si el teu nou tractament alternatiu és millor que res. Volem saber si és millor que el millor tractament de què disposem actualment. I malgrat això, repetidament veiem gent que encara fa proves comparant amb un placebo. I pots obtenir una llicència per treure la teva medicina al mercat amb dades que només mostren que és millor que no res, la qual cosa és inútil per un metge com jo que vol prendre una decisió.
So firstly, trials against placebo: everybody thinks a trial should be a comparison of your new drug against placebo. But in a lot of situations that's wrong; often, we already have a good treatment currently available. So we don't want to know that your alternative new treatment is better than nothing, but that it's better than the best available treatment we have. And yet, repeatedly, you consistently see people doing trials still against placebo. And you can get licensed to bring your drug to market with only data showing that it's better than nothing, which is useless for a doctor like me trying to make a decision.
Però aquesta no és l'única manera de manipular les dades. També pots manipular dades comparant la teva nova medicina amb una cosa realment inútil. Pots donar una dosi massa baixa del medicament competidor, perquè la gent no sigui tractada com cal. Pots donar una dosi massa alta del medicament competidor, per causar efectes secundaris. I això és precisament el que va passar amb una medicació antipsicòtica per a l'esquizofrènia. Fa 20 anys, va aparèixer una nova generació de medicaments antipsicòtics i el que prometien era tenir menys efectes secundaris. Així que es van començar a fer proves dels nous medicaments comparant-les amb els antics, però van donar els medicaments antics en una dosi ridículament alta: 20 mil·ligrams diaris d'haloperidol. I és una conclusió previsible, si dones un medicament en una dosi tan alta, que causarà efectes secundaris i farà que el teu nou medicament quedi molt bé.
But that's not the only way you can rig your data. You can also rig your data by making the thing you compare your new drug against really rubbish. You can give the competing drug in too low a dose, so people aren't properly treated. You can give the competing drug in too high a dose, so people get side effects. And this is exactly what happened with antipsychotic medication for schizophrenia. Twenty years ago, a new generation of antipsychotic drugs were brought in; the promise was they would have fewer side effects. So people set about doing trials of the new drugs against the old drugs. But they gave the old drugs in ridiculously high doses: 20 milligrams a day of haloperidol. And it's a foregone conclusion if you give a drug at that high a dose, it will have more side effects, and your new drug will look better.
Fa 10 anys, la història es va repetir quan la patent de la risperidona, el primer d'aquests nous antipsicòtics, va expirar, i tothom va poder copiar-la. Tothom volia demostrar que el seu medicament era millor que la risperidona, així que hi va haver un munt de proves de nous medicaments antipsicòtics comparant-los amb 8 mil·ligrams diaris de risperidona. De nou, no una dosi absurda, ni il·legal, però molt més alta del normal. Així segur que el teu nou medicament semblarà millor. Per tant no és sorprenent que, en general, les proves finançades per la indústria donen quatre vegades més sovint resultats positius que les proves finançades de manera independent.
Ten years ago, history repeated itself, when risperidone, the first of the new-generation antipsychotic drugs, came off copyright, so anybody could make copies. Everybody wanted to show their drug was better than risperidone, so you see trials comparing new antipsychotic drugs against risperidone at eight milligrams a day. Again, not an insane dose, not an illegal dose, but very much at the high end of normal. So you're bound to make your new drug look better. And so it's no surprise that overall, industry-funded trials are four times more likely to give a positive result than independently sponsored trials.
Però... i és un gran però... (Rialles) resulta que quan mires els mètodes utilitzats en proves de la indústria, de fet són millors que els de les proves independents. Així i tot, sempre se les arreglen per obtenir el resultat que desitgen. Com pot ser? Com es pot explicar aquest estrany fet? Resulta que el que passa és que les dades negatives desapareixen en combat; s'amaguen dels metges i dels pacients. I aquest és l'aspecte més important de tota la història. És el cim de la piràmide de l'evidència. Necessitem tenir totes les dades de cada tractament per saber si és o no efectiu de debò. I hi ha dues maneres diferents de veure si hi ha dades desaparegudes en combat. Pots utilitzar estadístiques o històries. Personalment prefereixo les estadístiques, per tant començaré amb elles.
But -- and it's a big but -- (Laughter) it turns out, when you look at the methods used by industry-funded trials, that they're actually better than independently sponsored trials. And yet, they always manage to get the result that they want. So how does this work? (Laughter) How can we explain this strange phenomenon? Well, it turns out that what happens is the negative data goes missing in action; it's withheld from doctors and patients. And this is the most important aspect of the whole story. It's at the top of the pyramid of evidence. We need to have all of the data on a particular treatment to know whether or not it really is effective. There are two different ways you can spot whether some data has gone missing. You can use statistics or you can use stories. I prefer statistics, so that's what I'll do first.
Això s'anomena gràfic en embut. I un gràfic en embut és una manera molt intel·ligent de veure si petites proves negatives han desaparegut en combat. És un gràfic de totes les proves que s'han fet d'un tractament en concret. Quan puges fins a dalt del gràfic, veus que cada punt és una prova. En pujar, aquestes són proves més grans, amb menys grau d'error. Per tant, són menys susceptibles de ser falsos positius o falsos negatius aleatoris. Així tots s'agrupen. Les proves grans estan més a prop de la resposta real. Si baixes cap a la base, el que trobes, en aquest costat, són falsos negatius espuris, i en aquest costat, falsos positius espuris. Si hi ha un biaix de publicació, si les petites proves negatives han desaparegut en combat, ho pots veure en un d'aquests gràfics. Aquí podeu veure que les petites proves negatives que haurien de ser a baix a l'esquerra han desaparegut. Aquest gràfic demostra la presència d'un biaix de publicació en estudis de biaixos de publicació. I aquesta és la broma més graciosa de l'epidemiologia que sentireu mai.
This is a funnel plot. A funnel plot is a very clever way of spotting if small negative trials have disappeared, have gone missing in action. This is a graph of all of the trials done on a particular treatment. As you go up towards the top of the graph, what you see is each dot is a trial. As you go up, those are bigger trials, so they've got less error; they're less likely to be randomly false positives or negatives. So they all cluster together. The big trials are closer to the true answer. Then as you go further down at the bottom, what you can see is, on this side, spurious false negatives, and over on this side, spurious false positives. If there is publication bias, if small negative trials have gone missing in action, you can see it on one of these graphs. So you see here that the small negative trials that should be on the bottom left have disappeared. This is a graph demonstrating the presence of publication bias in studies of publication bias. And I think that's the funniest epidemiology joke you will ever hear.
Així és com ho pots demostrar estadísticament, però què hi ha de les històries? Doncs són atroces, de debò. Hi ha un medicament anomenat reboxetina. És un medicament que jo mateix he receptat a pacients. I sóc un metge molt estudiós. Crec que intento fer tot el possible per llegir i entendre tota la bibliografia. Vaig llegir-ne les proves. Totes eren positives. Totes estaven ben fetes. No hi vaig trobar cap error. Per desgràcia, resulta que moltes d'aquestes proves s'havien amagat. De fet, un 76% de totes les proves realitzades sobre aquest medicament s'havien amagat dels metges i pacients. Si hi penses, si llancés una moneda 100 vegades, i pogués amagar-te'n el resultat la meitat de vegades, podria convèncer-te que tinc una moneda amb dues cares. Si traiem la meitat de les dades, mai podem saber quins són els efectes reals d'aquests medicaments.
(Laughter) That's how you can prove it statistically. But what about stories? Well, they're heinous, they really are. This is a drug called reboxetine. This is a drug which I, myself, have prescribed to patients. And I'm a very nerdy doctor. I hope I go out of my way to try and read and understand all the literature. I read the trials on this. They were all positive, all well-conducted. I found no flaw. Unfortunately, it turned out, that many of these trials were withheld. In fact, 76 percent of all of the trials that were done on this drug were withheld from doctors and patients. Now if you think about it, if I tossed a coin a hundred times, and I'm allowed to withhold from you the answers half the times, then I can convince you that I have a coin with two heads. If we remove half of the data, we can never know what the true effect size of these medicines is.
I aquesta no és una història aïllada. Aproximadament la meitat de les dades d'assaigs d'antidepressius s'han amagat, però encara va més lluny. El Centre Cochrane Nòrdic volia aconseguir les dades sobre això per posar-ho tot junt. Els grups Cochrane són una organització internacional sense ànim de lucre que fa revisions sistemàtiques de totes les dades aparegudes. I necessiten poder accedir a totes les dades de les proves. Però les companyies els amaguen dades, i també ho va fer l'Agència Europea de Medicaments durant tres anys.
And this is not an isolated story. Around half of all of the trial data on antidepressants has been withheld, but it goes way beyond that. The Nordic Cochrane Group were trying to get ahold of the data on that to bring it all together. The Cochrane Groups are an international nonprofit collaboration that produce systematic reviews of all of the data that has ever been shown. And they need to have access to all of the trial data. But the companies withheld that data from them. So did the European Medicines Agency --
És un problema que ara mateix no té solució. Per mostrar fins on pot arribar, hi ha una medicina anomenada Tamiflu, en la qual governs de tot el món s'han gastat milions i milions de dòlars. I s'han gastat els diners perquè els prometien que aquesta medicina reduiria la quantitat de complicacions de la grip. Ja tenim les dades que mostren que redueix la durada de la grip en unes hores. Però això no m'importa gaire. Als governs no els importa. Ho sento molt si tens la grip, sé que és horrible, però no ens gastarem milions de dòlars per intentar reduir la durada dels símptomes de la teva grip en mig dia. Receptem aquestes medicines, les acumulem per a emergències, perquè se suposa que reduiran el nombre de complicacions, és a dir, la pneumònia i la mort. El Grup Cochrane de Malalties Infeccioses, amb seu a Itàlia, ha estat intentant aconseguir totes les dades en forma utilitzable de les companyies farmacèutiques per poder prendre una decisió completa sobre si aquesta medicina és efectiva o no, i no han pogut aconseguir aquesta informació. Indubtablement, aquest és el problema ètic més important a què s'enfronta avui la medicina. No podem prendre decisions en absència de tota la informació.
for three years. This is a problem that is currently lacking a solution. And to show how big it goes, this is a drug called Tamiflu, which governments around the world have spent billions and billions of dollars on. And they spend that money on the promise that this is a drug which will reduce the rate of complications with flu. We already have the data showing it reduces the duration of your flu by a few hours. But I don't care about that, governments don't care. I'm sorry if you have the flu, I know it's horrible, but we're not going to spend billions of dollars trying to reduce the duration of your flu symptoms by half a day. We prescribe these drugs. We stockpile them for emergencies on the understanding they'll reduce the number of complications, which means pneumonia and death. The infectious diseases Cochrane Group, which are based in Italy, has been trying to get the full data in a usable form out of the drug companies, so they can make a full decision about whether this drug is effective or not, and they've not been able to get that information. This is undoubtedly the single biggest ethical problem facing medicine today. We cannot make decisions in the absence of all of the information.
Així doncs, és una mica difícil extreure alguna conclusió positiva d'això. Però jo us diria: crec que la llum del sol és el millor desinfectant. Tot això està passant a plena vista, i tot està protegit per un camp de força de tedi. I crec que, amb tots els problemes de la ciència, una de les millors coses que podem fer és aixecar la tapadora, remenar la mecànica i fer-hi un cop d'ull.
So it's a little bit difficult from there to spin in some kind of positive conclusion. But I would say this: I think that sunlight is the best disinfectant. All of these things are happening in plain sight, and they're all protected by a force field of tediousness. And I think, with all of the problems in science, one of the best things that we can do is to lift up the lid, finger around at the mechanics and peer in.
Moltes gràcies.
Thank you very much.
(Aplaudiments)
(Applause)